https://habr.com/en/company/klinika_shilovoy/blog/510684/- Клиника офтальмологии доктора Шиловой corporate blog
- Biotechnologies
- Lazers
- Health
he first symptoms are near vision loss. Objects at close examination blur. Woman struggles to cope with manicure. A man goes fishing and there he understands that he puts the worm with difficulty. And at the same time, a distant view, as it were, has not changed. Traditionally, this condition is called “short arm disease” — it seems that the vision is good, but the length of the arms is not enough for clarity close. This is for those over 40.
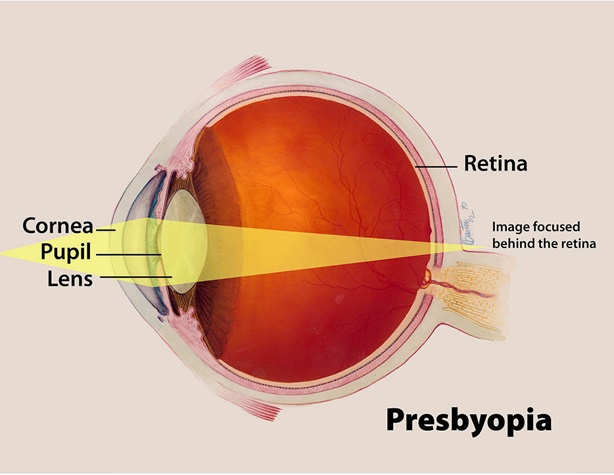
This is presbyopia. With age, a person’s vision in terms of ease of focusing at different distances deteriorates. The exact reasons for this “depreciation” of the visual apparatus are still being investigated: it is known, for example, that this mechanism works only in higher primates. Dogs and cats have no presbyopia, monkeys have it. By the way, this is partly why presbyopia is difficult to study: to study dynamic refraction (accommodation), a living object is needed.
The lens thickens and becomes less elastic, the ligamentous apparatus suffers, the muscles lose their ability to act as before — presbyopia occurs. Until recently, the theory of accommodation of the German physician Helmholtz, put forward in the 19th century, which only affects the lens and its ligamentous apparatus, was recognized as the only correct one, but more recent studies say that all the eye structures are involved — the cornea, vitreous body and even the retina. The result of presbyopia is the loss of the ability to accommodate, that is, the ability to view objects at different distances without additional correction.
When Presbyopia Appears
The average age of appearance of the first symptoms — 40 years, rarely later — I had patients who, even at the age of 50, felt quite comfortable, but by the age of 60-70, they began to suffer from presbyopia (in combination with cataracts). Presbyopia is considered to be the same natural physiological process as the appearance of wrinkles or gray hair with age.
In my practice, patients are very weak about what is happening. Almost everyone complains that «I have ruined my eyesight with a computer.» No, everything is easier. You've gotten older.
How does this affect those with myopia, hyperopia or astigmatism? In a person with one hundred percent vision (not important, natural or after laser correction, or with an implanted intraocular lens) objects near start to blur. The text in front of the nose is not visible either at 8 centimeters, or at 15 — but already somewhere far away. To read you need glasses for near. Eyesight does not deteriorate. Points for distance, if any, remain the same.
Nearsighted with weak minus and without pronounced astigmatism may keep the ability to read without glasses longer, although the points for the distance will not disappear. Moreover, they will interfere when working close, they will need to be removed. Ease of focusing on previous glasses or contact lenses will fade. By the years of 50-60, another pair of points will appear with a small plus now. In short, plus a minus does not go to zero.
If myopia is stronger, a second pair of glasses is needed, weaker to read and do petty work. As a result, by the same 50-60 years there will be 3 pairs of points — the strongest ones at a distance, weaker by 1-1.5 diopters by an average distance and weaker by 2-2.5 for reading and near. In general, there are not many “minuses” in the minus.
Long-sighted people feel the symptoms of presbyopia even earlier — after the age of 35. This is because a plus for accommodation is added to its advantage. As a result, having worn glasses for reading for a couple of years, they begin to notice that these glasses suddenly become visible and clearly visible, and for a near distance an even stronger correction is required. And such patients run to an ophthalmologist with the story that a computer, or books, or a job “messed up” their eyes. And they do not always believe the story that changes in such a plan are irreversible and incurable with drops, miracle pills, strengthening super exercises, sentences and urine of a young piglet.
As a result, long-sighted people after 40 years acquire reading glasses, while somehow maintaining the ability to see well in the distance. Somewhere after 50, after an unsuccessful struggle with presbyopia, they still put on two or three pairs of glasses or progressive lenses, or seek surgical help.
Worst of all astigmata — the picture quality is bad at all distances. Therefore, the higher the degree of astigmatism, the more binding to the points. In the end, it all ends with a few pairs of points.
If you have ever had an eye examination with pupil dilation (before the first prescription of glasses, before surgery, when examining the fundus of the eye and so on) — the first hour after the drug treatment you just get a simplified presbyop simulator. The only difference is that everything around will not seem so unbearably bright.
How does this affect vision correction and laser surgery in youth?
The first case: a patient aged 18 years (before that, the eye is still actively developing) to about 40 years. In this situation, the choice is a complete correction. At the age of over in the absence of other problems that may appear at this point (cataract, glaucoma, dystrophy of the retina, etc.), we allow for presbyopia.
In any case, after laser correction to emmetropia (the state when the image falls into the retina), any optics become close to normal. This translates a person into a standard peer-presbyop, eliminates the need to wear glasses for distance and gives a comfortable feeling in everyday life. And presbyopia should be taken as a given age.
If you want to reduce dependence on presbyopia, we find compromise surgical options. There are a lot of them, about this later in the text and in previous posts.
And if I already have presbyopia?
If the patient is already with presbyopia and a few pairs of glasses completely suits him, then in this situation we say: if you are satisfied with glasses, this is not a disease. Go, try. But many are not ready, and really want to make a correction. This is especially true for women — there is a certain stereotype that a woman who puts on reading glasses is already a grandmother (positive glasses are always made with large glasses or, even more old, are worn “on the nose”). Athletes and people with an active lifestyle also willingly go for a correction.
Correction is done according to needs. We ask in detail about the occupation of a person and his hobby. For example, if a patient is a jeweler or embroiders, a close focus is needed. The patient is doing research with the selected focal length, he assesses how comfortable he is. As a result, the optimal method is chosen.
Since different tasks require different focal lengths (simplifying them, three: close focus — reading, embroidery, medium distance — computer, music stand, easel, far focus — driving, theater, etc.), several techniques can be applied. I will not write about the methods that have been experimentally conducted over the past 20 years — laser and scalpel notches, implantation of rings and accommodating lenses, etc., which showed its inconsistency. Here are the options:
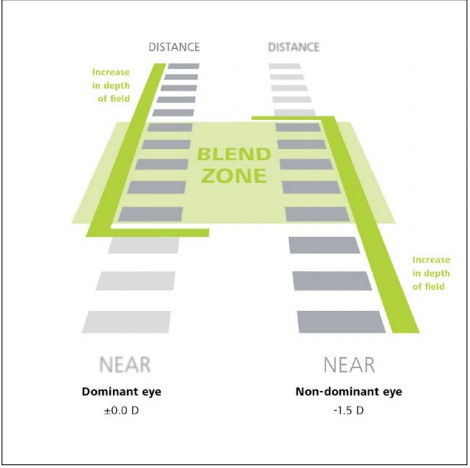
1. Monovision method. Two eyes are adjusted differently: one for near, the second for distance with a difference of about 1-1.5 diopters. The leading eye helps to see into the distance, the uninformed — close. Since not every brain can get used to this, tests with glasses or lenses are necessarily made until the patient is convinced that such a method is suitable for him. The essence is very simple — you need to learn how to switch the driven and leading eyes at different distances of the object. The brain does it automatically.
This method is available for both glasses and contact lenses, phakic intraocular lenses, artificial lenses and laser correction.
This is the principle of monovision.
2. Undercorrection during laser surgery. It's simple — a patient with a vision of -6 diopters gets a correction of up to -1 diopters, and as a result can be relatively comfortable and drive a car and read. The type of laser correction does not matter, of course, under equal conditions, I am for the SMILE technology as the most progressive and safe. You can read about it in detail
here.
The method is also available for all types of correction.
3. Laser correction with presbyopic profile (with multifocal cornea) — PresbyLASIK. With the laser cornea, you can cut almost any complex shape with filigree precision, so you can make a lens that will have several focal lengths. The roughest approximation is that the Fresnel lens is applied to the eye (although, of course, modern profiles are much more difficult). Payback is much more beautiful aberrations. Each manufacturer of lasers comes up with their own profiles and methods for creating them. Still, the market is huge — one hundred percent of patients are their consumers. Therefore, the best minds are working on this.
The bad thing is that in such a situation an irregular cornea is made. That is, then it is more difficult to calculate the artificial lens, while we can not take into account these irregularities. And somewhere in 5-10 years, it is certain that a re-correction is needed — the presbyopia is developing. The patient may feel chromatic distortion, coma. The rays on the retina are focused not to a point, but to a smeared block, or to a star spot.
This is what a multifocal cornea looks like.
4. There is another alternative: introducing a special lens directly into the cornea with a hole in the center. In fact, it is the installation of the diaphragm. That is, increasing the depth of the sharply displayed space by reducing the amount of light falling on the retina — we leave only those rays that go through the center of the lens of the eye. In Russia, these lenses are not yet certified. In the world put quite active. The reviews are different, they are not recommended in our German clinic. Of the obvious drawbacks — interfere with optical side effects, heavier at dusk.
five.Implantation of multifocal phakic lenses. The technique is similar to the operation with refractive phakic IOLs. As a result, the cornea and its own lens are preserved. They do not interfere with the work of the eye until the cataract is ripe. But they are not suitable for everyone in terms of anatomical parameters — the distance between the iris and the lens. The lens grows, not everyone has enough space for an implant in the back chamber of the eye. In this case, it is necessary to take into account the width of the pupils of the patient, otherwise aberrations due to multifocal optics may also interfere.
How this happens, you can read in a post about the types of correction and the continuation of the eye and its biomechanics:
here.
The bottom line is that we cannot make the presbyopic eye with the eye of a 20-year-old person. Any choice is a compromise between picture quality, convenience and the ability to see near objects.
What exactly does not help?
1. No drops, pills (even large and red), dark rituals and folk methods to correct presbyopia. But obscurantism wins, so the people believe in it. And asks for a pill so that everything goes by itself. Doctors in clinics sometimes meet, relying either on the placebo effect, or on the premium pharmacy for the plan for the sale of drugs. And the Internet is “teeming with” sentences like without the operation “make from -5 to 1”, “read without glasses until old age” and “see through the walls”. By the way, often for very big money.
2Exercises of the muscles of the eyes can slightly improve vision (in general, it is better to do “exercises” for the eyes and being a healthy person), partially eliminate the effects of fatigue or muscle spasm (as a rule, it is not at this age). But nothing can be done with presbyopia systemically. However, you can try to work an hour a day every day. It will not be worse. Often, in order not to wear glasses for near, such tricks are used, such as highlighting the menu in a restaurant with a mobile phone, buying a phone with larger buttons, increasing the font on an electronic screen, etc.
How to measure accommodation and calculate presbyopia?
To calculate the reserve of accommodative abilities for being close to the patient, the text is given, located at a distance of 33 cm from the eyes. Each eye is examined in turn. After that, lenses are placed in front of him: the strength of the maximum positive lenses with which text can be read will be the negative part of the relative accommodation. The use of positive lenses causes a decrease in the tension of the ciliary muscle.
The strength of the maximum negative lenses with which text reading is still possible determines the positive part of the relative accommodation, the use of negative lenses causes additional strain on the ciliary muscles, this part of the accommodation is also called the margin or positive reserve of relative accommodation. The sum of the positive and negative parts (without taking into account the sign of the lenses) shows the amount of relative accommodation.
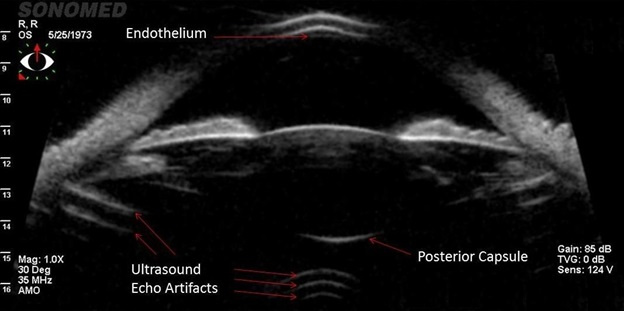
As the body ages, the reserve capacity of accommodation gradually decreases. So, according to Donders, in patients with normal vision at 20 years old, it is about 10 diopters, at 50 it drops to 2.5 diopters, and by the age of 55 to 1.5 diopters. There are modern devices that automatically measure static refraction and dynamic refraction (accommodation). And we can observe “live” this process during UBM (ultrasound biomicroscopy), where we observe the state of the lens and its ligaments.
For the correction of presbyopia all the same optical glasses are used for proximity. To determine their strength, the formula is used: D = + 1 / R + (T-30) / 10.
In it, D is the size of the glass in diopters, 1 / R is the refraction for correcting the patient's optics (nearsightedness or farsightedness), T is the age in years.
Here is the practical calculation of this indicator for a patient of fifty years.
If a person has normal vision, D = 0 + (50-30) / 10, that is +2 diopters.
With myopia (2 diopters) D = -2 + (50-30) / 10, that is, 0 diopters.
With farsightedness in 2 diopters, D = + 2 + (50-30) / 10, that is, 4 diopters.
Isn't that exactly CVS?
Symptoms in computer vision syndrome (CVS) may be the same as in early presbyopia. Naturally, it is necessary that you looked ophthalmologist. However, if you are over 40 — 99.9%, that is not CVS.
There are several pathological, but temporary changes in accommodation, these include accommodation spasm. Then we are talking about a spasmodic enhancement of the refraction of the eye, which is associated with the absence of relaxation of the fibers of the ciliary muscle. At the same time, we determine a sharp decrease in visual acuity (especially in the distance) and visual performance in general. By the way, such a condition can be easily obtained in case of poisoning with organophosphorus agents and some drugs.
There is also the concept of customary-excess voltage of accommodation — PIN. It causes an enhancement of the initial refraction of the eye (more often in children), which can progress at different speeds. This condition is provoked and maintained by the wrong mode of visual activity, especially at close range.
Uncorrected long-sighted people often have accommodative asthenopia, a condition in which there is rapid fatigue of the eye apparatus during work.
Accommodation paralysis is accompanied by focusing the eye on its furthest point. The distance it depends on the initial parameters of the refraction. Paralysis can also occur against the background of general body poisoning (for example, with botulism) and with the use of certain drugs.
And presbyopia implies an age-related decline in accommodative abilities, characteristic of people over 35-40 years old.
What happens next as presbyopia develops and is closer to cataracts? Presbyopia progresses with time, it reaches its maximum in 60-70 years and eventually flows into a cataract. If opacities appear in the lens — the quality and quantity of vision noticeably decrease. And the question naturally arises of lens surgery, replacing it with a new one. I told about this in previous posts about cataracts and artificial lens.
In short, if the new lens is single-focus, then you still need glasses for some distance, if multifocal — you get maximum independence from the glasses. Again, you can consider the option of monovision.
It is important that in no case do you need to wait for the maturation of a cataract, and it is necessary to part with it when it begins to interfere. The choice of an artificial lens is a strictly individual task, which only surgeons with a great deal of knowledge and experience in implanting various IOL models can do.
Total
Accommodation is still being studied, since it is not fully understood how it works. For example, about 5% of patients and an artificial monofocal lens can get the so-called “accommodation of a pseudofack eye,” that is, they will learn to change the focal length of the lens. How to repeat this is not clear. Therefore, it is quite possible that in the future we will see serious progress on this topic. However, in the perspective of 10 years there is nothing serious yet, alas, not — we follow all clinical trials very carefully.